
Why Coronary Artery Calcium Tests Reveal Many Athletes Have Calcified Arteries
It is more common now for the over forty crowd to get a coronary artery calcium scan as part of cardiovascular risk assessment. Because of this, more athletes over forty are discovering that they have coronary artery disease. Deciding what to do with this information and producing a customized treatment plan is the main focus of my practice. I have been practicing preventive cardiology for twenty years and, being based in Boulder, CO, have had the privilege of seeing a large number of elite masters age athletes who have made this anxiety producing discovery while in my care.
In the last ten years there has been an uptick on articles in medical literature reporting arterial plaque (atherosclerosis) in experienced male endurance athletes. Women get coronary calcium too, but it happens about seven to ten years later than in men and for this reason there is not as much data. Unfortunately, women may catch right up to men at an accelerated pace after menopause. It’s worth mentioning that more women die of heart attacks than breast cancer.
CAC Tests Show Male Endurance Athletes May Have More Arterial Plaque
Male endurance athletes may have more arterial plaque as determined by a coronary artery calcium (CAC) test, also generally known as a “heart scan”.² A CAC is like a fancy x-ray of the heart, using computed tomography (CAT scan). Arteries develop calcium deposits at varying degrees because of atherosclerosis. The calcium is as easy to see with an x-ray as bones are. Generally speaking, the more plaque, the more calcium, and vice versa. The CAC test is inexpensive, and I suggest that men over forty and women over fifty have the test done.
Arterial plaque causes most heart attacks . . . especially when it ruptures. Blocked arteries always cause some type of symptom such as fatigue or pain. There is an exception though. If the collateral circulation is extensive enough the patient may not have any symptoms.
Vulnerable plaque is the worst . . . it is unstable and can rupture, thus clogging an artery downstream. Both higher CAC scores and reduced cardiovascular fitness are strong predictors of future cardiovascular events such as stroke and heart attack. Coronary calcium is an indirect measure of arterial plaque. The scan cannot tell the difference between stable and unstable plaque but is still a good test for many reasons. It is used to determine risk but can also be used to follow plaque progression or regression over time. This is a good test to perform in people without symptoms to determine if they should be treated. Patients with chest pain either with or without exercise should be getting a full work-up at the cardiologist first and then do the CAC test later.
Coronary artery calcium scoring is a helpful test, but it does not measure how old the plaque is, the degree of blockage, or measure new plaque. The only way to track progression is to do coronary artery calcium scoring every one to three years. There is a workaround for detecting vulnerable plaque and it is called a carotid intima media thickness test. I do these on all my patients as well as other tests to see if the plaque is the risky type.
Evaluating Arterial Plaque in Runners
The association between arterial plaque and extreme exercise began around 2008 when it was discovered that there was more coronary calcium in runners than non-runners. It was not clear as to why. It was postulated that it could be personality type, past diet, and/or lifestyle factors. A follow-up study showed that plaque could increase in runners who did the Race Across America proving a direct link between extreme exercise and atherosclerosis. The Race Across America is a 140-day running race. They run 25 miles a day. Subjects were evaluated before the race and afterwards. Eight of the ten runners finished the race. One woman and three of men had plaque before the race and the plaque increased in all four of these runners. None of the runners without plaque prior to the race developed any plaque. This study supported the possibility that extreme amounts of exercise could accelerate plaque growth directly. ³
Potential Causes of Increased Arterial Plaque from Exercise
One cause of increased arterial plaque from exercise could be that exercise increases parathyroid hormone, and parathyroid hormone increases blood levels of calcium. Another possibility could be that inflammation from muscle damage might also damage the endothelium. The endothelium is the first line of defense for an artery. When it is disrupted or damaged, plaque begins.
My hypothesis is that runners are at greater risk because of the high impact nature of the sport, especially as compared to cycling or swimming. I think that mechanical stress from millions of foot strikes (shaking) plus a fast-beating heart play a role. The additional shaking from running may also cause microscopic endothelial damage. Another idea is that the oxidative stress caused by high intensity long duration endurance exercise is to blame. It’s quite possible that all these factors play a role.
Past Studies on the Effects of Exercise on the Heart
In 1899 there was a study published called “Adverse Effect of Violent and Prolonged Muscular Exercise Upon the Heart”. In this study, it was postulated that inflammation from muscle damage was to blame. Through studying runners at the Boston Marathon using blood testing, it was shown that post race inflammation markers were like someone who is having a heart attack! Adequate intake of fruit and vegetables helps prevent this, along with other nutritional supplements like antioxidants and essential amino acids.
As part of my masters athlete physicals I check these inflammation markers along with other blood tests such as cardiac enzymes and additional biomarkers associated with cardiac strain and endothelial health.
The Importance of Calcium Density in Endurance Athletes
Even very fit exercisers can get increased calcium density in arterial plaque. This may make it more stable. This is a complicated issue because although an increasing coronary calcium score is associated with more risk, increased density of the plaque decreases this risk. However, the only way to really see the density is to get something called a CT angiogram. Studies have found that athletes generally have increased calcium density and more stable plaque.4 It’s not easy to know if this is happening or not without further testing.
This brings up the issue regarding the incidence of heart attacks during races. Although small, there is an increased risk of a heart attack during a race, but the more physically fit you are, the lower the risk. Even though there might be more arterial plaque and more calcium present, athletic people have less heart attacks and live longer. It is also entirely possible to have no calcified plaque and be largely genetically protected from atherosclerosis.
When we exercise, our hearts become stronger, and the blood supply increases due to more vascularization. This is called collateral circulation and is an adaptive mechanism. The heart, being a muscle, responds a lot like skeletal muscle. The harder you work, the stronger it gets. With increased oxygen requirements, the heart responds by growing more arteries, often bypassing diseased arteries. There is a benefit to this. The chance of survival would be much higher because there is more blood supply and oxygen.
All data supports the fact that physically fit populations have less “all-cause mortality” which includes cancer, stroke, and fatal heart attacks. Regardless of this encouraging news, anyone with coronary calcium should get a complete work-up because heart attacks can and do happen to healthy people!
Analyzing the Latest Studies of Intense Exercise and Cardiovascular Health
In a recent study published in the Journal of the American Medical Association (JAMA), Dr. Benjamin Levine helps clarify the issue. He studied 21,000 healthy men, ages 40-80, between 1998 and 2013. The study subjects underwent coronary calcium testing. Most were runners but some were also swimmers, cyclists, rowers, and triathletes. He found that extreme exercise does not increase risk of heart attack and stroke. This is certainly good news for those of us who like intense exercise. Paul Thompson MD at Hartford Hospital has done a lot of work on this as well. He found that fitness mitigates the risk.
Male Endurance Athletes Have Less Rupture Prone, Dangerous Plaque Compared to Sedentary Controls
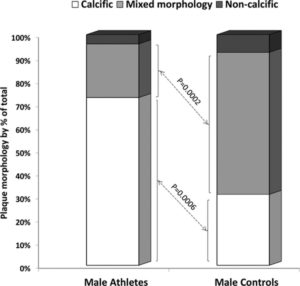
From: Prevalence of Subclinical Coronary Artery Disease in Masters Endurance Athletes With a Low Atherosclerotic Risk Profile. Circulation. 2017;136:126–137. In this study, athletes older than 40 with atherosclerotic risk factors for coronary artery disease report higher coronary artery calcium (CAC) scores compared with sedentary individuals. Calcified plaque is more usually more stable than mixed or non-calcified plaque! Masters athletes were >40 years of age, ran ≥10 miles or cycled ≥30 miles per week and have continued to do so for ≥10 years, and competed in ≥10 endurance events, including marathons (26.2 miles, 42.2 km), half marathons (13.1 miles, 21.1 km), 10 km races, or endurance cycling races ranging from 41.1 to 161.5 miles, 66 to 260 km) over a 10-year period.
Take Home Messages About Heart Health and CAC Tests
- The latest study by Levine et al. showed that a high level of endurance exercise does not raise heart attack risk even though there may be a higher CAC score. 5
- Consider low dose aspirin. A study published in February 2019 strongly suggested that aspirin could help reduce the incidence of heart attacks during running races. What they found though is an increased incidence of heart attacks in patients after they discontinued Aspirin helps reduce the viscosity of the blood by making platelets less sticky. It also lowers inflammation markers. 6
- Elite level male endurance athletes who have risk factors for atherosclerosis tend to have higher scores than sedentary controls, but less overall risk of dying of a heart attack.
- Get a coronary artery calcium test if you are a male over forty or a female over fifty.
- Knowing how to consult with athletes and interpret CAC tests is a specialty. Your primary care provider should not be expected to be an expert on this. Cardiologists know about coronary artery calcium scoring but may not be able to offer much more than cholesterol medication if you do not have any symptoms.
- Get a carotid intima media thickness test (CIMT). The company I use provides data on what the plaque looks like and whether it is new or old. Most of the companies will not provide this but will give you the arterial thickness which is also an indirect measure of arterial age.
- Follow a heart healthy diet. Say no to junk food, excess sugar, processed food, fried food, and high fat meat. Say yes to nutrient dense (not calorie dense) natural food like fruits, vegetables, healthy fats from plants, fiber, red wine, nuts, seeds, fungi, whole grains, fish, and lean meat. Eat real food, and mostly plants. You have heard all of this before, right?
- If you have pain with exercise, make an appointment with a cardiologist immediately. If you see a general practitioner, you will just be referred to a cardiologist anyway.
- See someone well versed in preventive cardiology (and ideally an athletic population as well) once you have your CAC test. Conventional doctors may not be well versed in the clinical utility of CAC tests and are more geared towards treating patients after symptoms start.
- Insurance does not cover a CAC test therefore it is an out-of-pocket expense costing between $100 and $200.
Is High Volume Endurance Exercise Safe?
According to the medical literature, high volume endurance exercise is safe, even when coronary calcium is present. This does not mean it safe for you, it just means that when they collect the data it shown to be generally safe. The amount and the density matters, in addition to other risk factors such as inflammation, poor diet, and unfavorable cholesterol. Many other risk factors may exist such as but not limited to: sleep apnea, hypertension, prediabetes, elevated small cholesterol particle size, and low HDL syndrome.
Coronary calcium scoring is not an exact science. More analysis needs to be done on high impact runners versus low impact athletes because the runners have more arterial calcification in comparison. Much should be considered when determining risk in an athlete (or anybody). An individualized, comprehensive workup needs to happen on anyone with elevated coronary calcium. Elite masters athletes are a rare breed and cardiologists encounter them infrequently by comparison to other people in the waiting room. A cardiology referral is not always necessary for something like this, but a patient should not expect their primary care doctor to be able to perform a comprehensive risk analysis. I only say this because it is a common complaint. Primary care doctors work awfully hard and have to follow strict guidelines (standard of care). They simply do not have the time, or are not reimbursed, for the type of work that needs to be done.
Schedule an appointment with Dr. Steve Parcell to discuss your heart health: 303.884.7557.
1 Too much exercise can damage the heart in other ways. While its normal for the heart to enlarge and adapt to high volumes of training it may not adapt in a healthy way, especially as we get older. Pathologic remodeling can include fibrosis, the wall of the heart muscle getting too thick and increased risk of electrophysiological problems like atrial fibrillation. Typically, an echocardiogram and electrocardiogram are needed to diagnose these conditions.
2 Coronary Artery Calcification Among Endurance Athletes “Hearts of Stone”. Circulation. 2017;136:149–151
3 Fitness, Exercise, and Coronary Calcification. Originally published18 Jun 2018. Circulation. 2018;137:1896–1898
4 Relationship between lifelong exercise volume and coronary atherosclerosis in athletes. Circulation. 2017;136:138–148
5 Association of All-Cause and Cardiovascular Mortality With High Levels of Physical Activity and Concurrent Coronary Artery Calcification. JAMACardiol. Published online January 30, 20194(2):174–181. doi:10.1001/jamacardio.2018.4628
6 Aspirin to Prevent Sudden Cardiac Death in Athletes with High Coronary Artery Calcium Scores. Am J Med. 2019 Feb;132(2):138-141